So, what exactly is acne?
Acne is one of the most common skin conditions I see, both in my GP clinic and through messages I get on Instagram. And yet it’s also one of the most misunderstood, mostly because people assume it’s a teenage problem, or a hygiene problem, or something you should just be able to clear up with a good cleanser. None of that is true.
Acne happens when hair follicles become blocked with oil and dead skin cells. That blockage creates the perfect environment for a bacteria called Cutibacterium acnes to multiply, which triggers inflammation. The result is everything from small whiteheads and blackheads through to deeper, painful cysts that can leave scarring if they’re not treated properly.
It can affect your face, chest, back and shoulders. It can start in your teens and clear up, or it can show up for the first time in your 30s. It can be mild and occasional or persistent and deeply affecting. I see patients who have had acne for twenty years and have tried everything. I also see teenagers who are mortified by a few spots and don’t know where to start.
Wherever you are on that spectrum, there is something that will help. The key is understanding what’s driving it for you.
And why does it happen?
Understanding what’s driving your acne matters because it shapes how you treat it. The same spot cream isn’t going to work the same way for a 16 year old with oily skin as it will for a 38 year old whose acne started after coming off the pill. There are four main drivers and most people with acne have a combination of them.
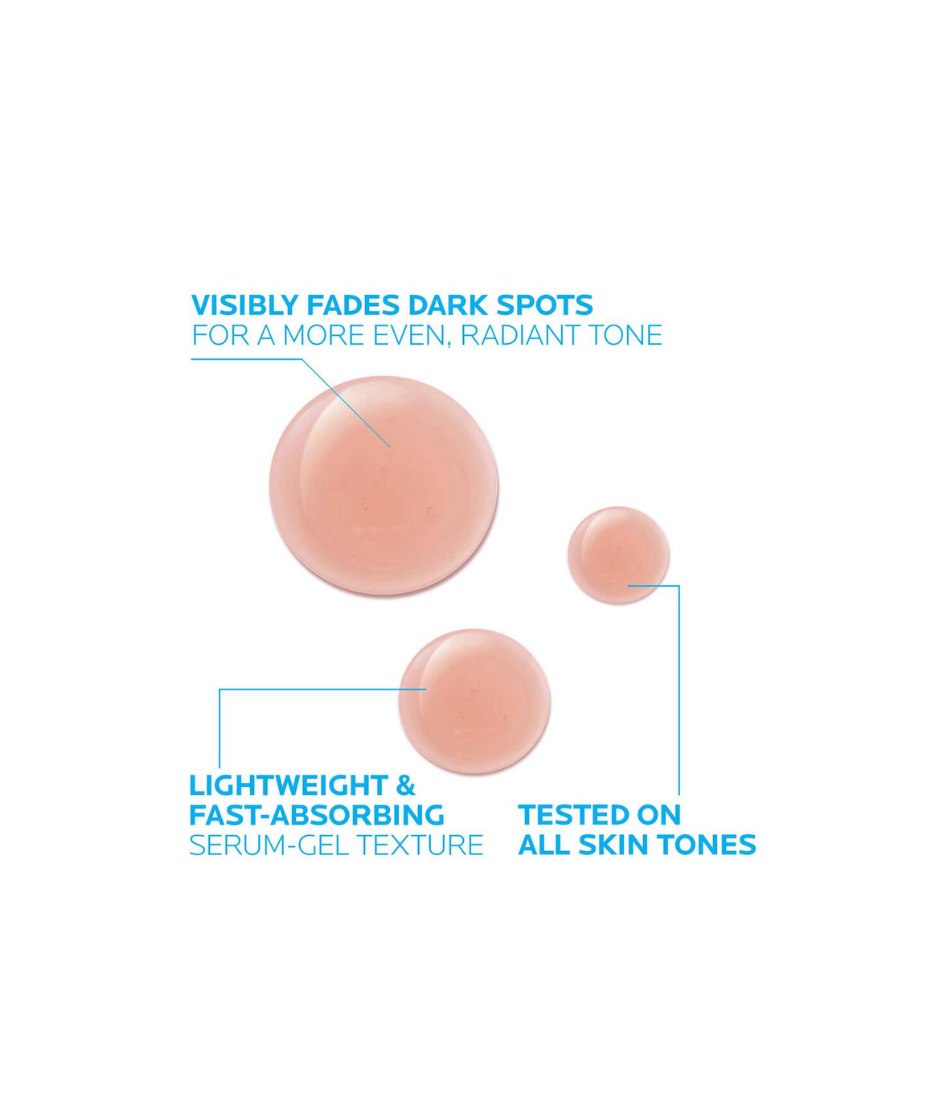
Excess sebum production.
Your skin produces oil naturally and needs it. But some skin, often genetically, produces more than it needs. That excess oil mixes with dead skin cells and blocks the follicle.
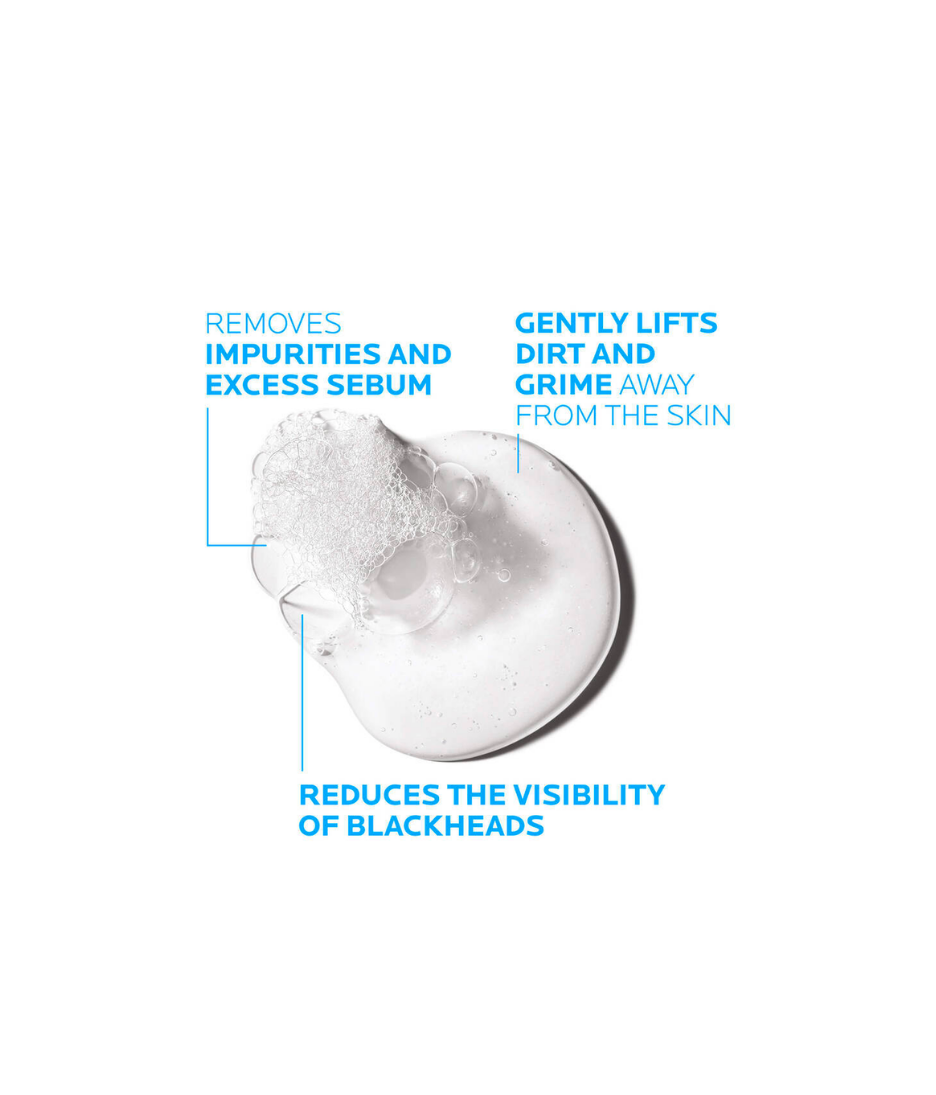
Dead skin cell buildup.
Skin sheds constantly but sometimes that process doesn’t happen efficiently enough and cells accumulate in the pore instead of shedding properly.
Bacteria.
Cutibacterium acnes lives on all of our skin but in a blocked, oily follicle it multiplies rapidly and triggers an immune response, which is what causes the redness and swelling.
Hormones.
This is the big one that gets underestimated, especially in adults. Androgens, which both men and women produce, stimulate the sebaceous glands to produce more oil. This is why acne often spikes around your period, during pregnancy, after coming off the pill, and in perimenopause. It’s also why stress makes acne worse, cortisol drives androgen production.